


The Big Lies that are Driving Canada's National Health Care Debate
The "adult conversation" we all need to have about health care in Canada: The market should not be able to legislate life and death.

When he became PC Premier of Manitoba in 2016, Brian Pallister launched a communications campaign that claimed that whatever was going wrong in health care was not his fault. It eventually became the national narrative for Canada’s Premiers.
Even as his government imposed freezes that directly led to lost positions and shuttered programs, the government made it part of their talking points to create the impression the federal government was cutting health care, when the province was.
The way they did this was by presenting a series of half-truths and by presenting facts stripped of context.
The techniques used were simple, and were repeated year after year, designed to manipulate and deceive the public.
Step 1: Promise provincial budget increases, while health actual spending was frozen
Budget Bait and Switch: Make an empty budget commitment to an increase for public relations purposes, then immediately clawing it back
By budgeting increases they have no intention of turning into actual spending, the government could credibly say the budget number wasn't lower than the previous year, even as closures, layoffs and service reductions in health care occurred as a result. The result was a misleading public denial of responsibility.
One of the routine gambits was to claim health care increases in the budget, then immediately turn around to the bureaucracy and demand cuts of 15% of the bureaucracy. As a consequence, the new health care spending never happened, for three years straight - from 2016/17 through to 2018/19.This declaration was in the Manitoba budget of 2019. A few weeks later, three hospital Emergency Rooms were closed.
This strategy - of promising big in the budget and immediately reneging, meant that the PCs could evade responsibility for service reductions and job losses in health care, and then, at the end of the year, boast of their progress in balancing the budget.

Step 2: While freezing their own health budgets, Premiers falsely suggested federal health funding was being cut
The Premiers and the Council of the Federation bought ads in newspapers across Canada, repeating a claim that the “need has never been greater” while “federal government funding has never been lower.”
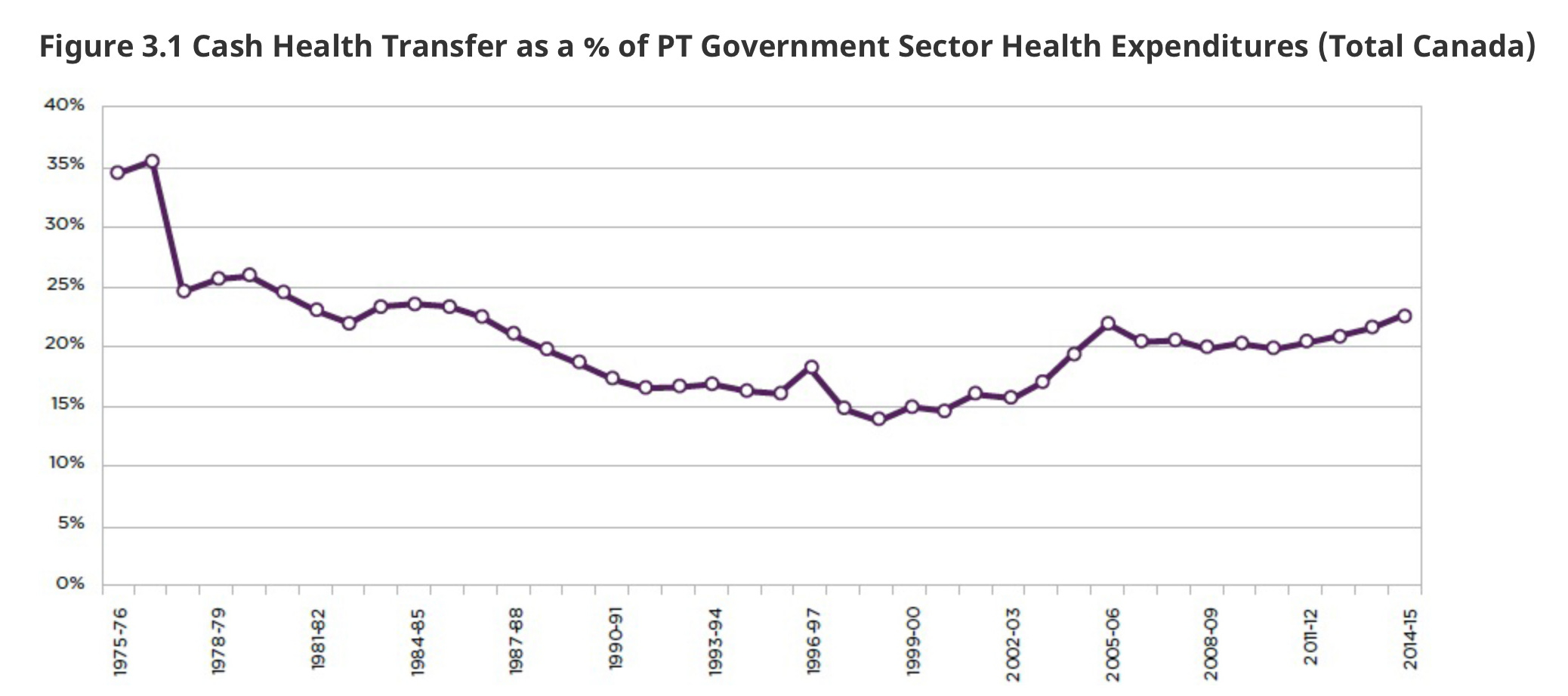
This was a simple claim- when Medicare started, that the federal government used to pay 50% of health care costs, now paid 22%. The impression is clearly that the reason health care was in such a mess was because the Federal government wasn’t funding it adequately.
This graph shows what actually happened - with CHT as a percentage.
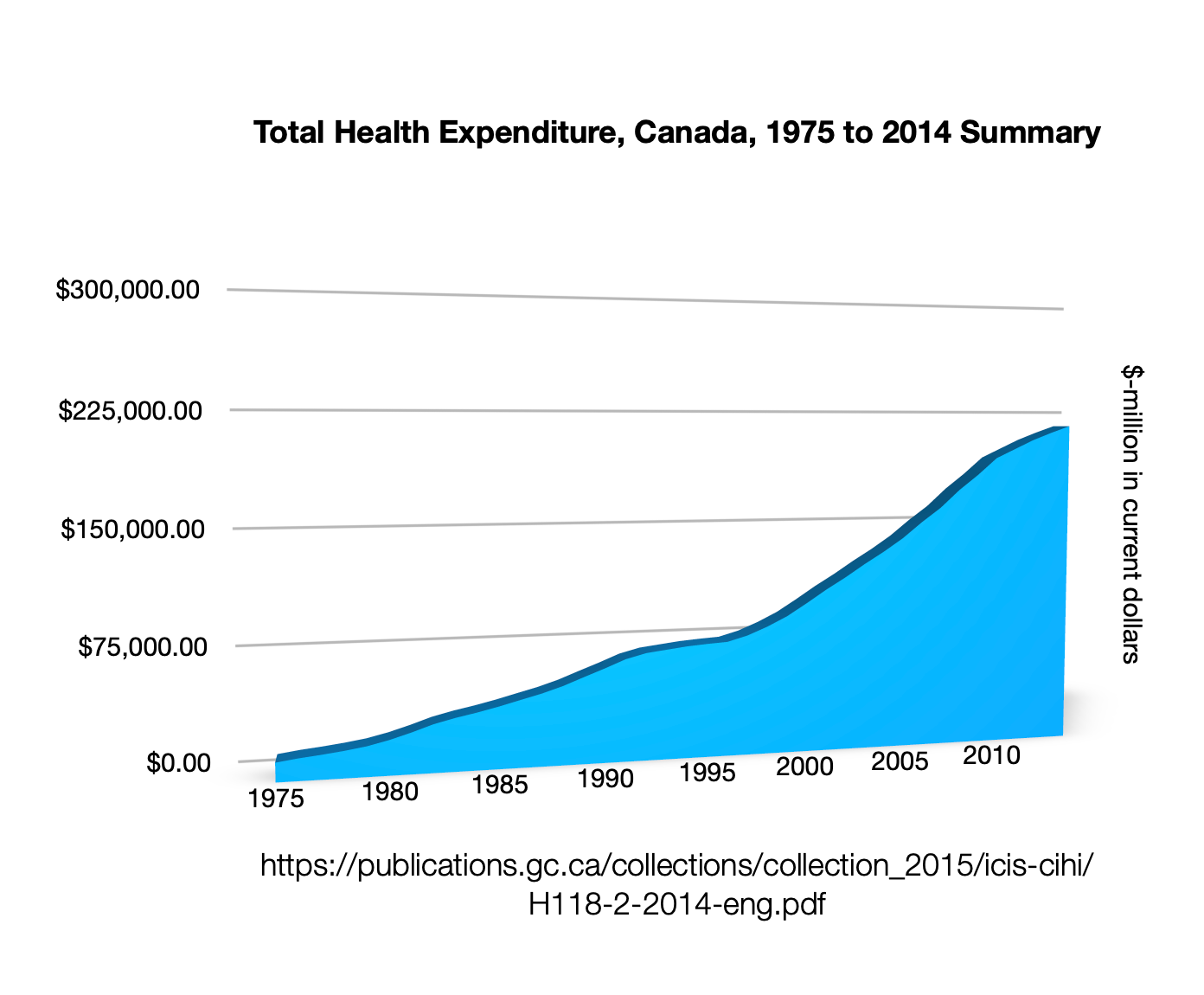
As does this one, with total health expenditures.
What it left out was that the last time the federal government paid 50% of the share was in 1976, when a new federal-provincial funding formula was introduced.
Taken together, these distortions were eventually adopted by all Premiers and the Council of the Federation, meant that provincial governments who were cutting or freezing health care budgets successfully shifted the blame to a federal government that was increasing federal transfers.
The reality is that it was Conservatives who cut and froze federal funding to health, especially to health care in Manitoba, then proceeded to make cuts at the provincial level.
It should be noted - this is a strategy similar to what some Republican states have done in the U.S. When the U.S. federal government expanded Medicaid, a program to help low-income Americans with health care costs, a dozen states refused to implement it. They were willing to deny improved health care to their own citizens, for political purposes,
One of the reasons Canada’s health care systems are at the breaking point is that provincial governments were similarly obstructionist.
For example, the PC Government in Manitoba dragged its heels on signing a $400-million fund for mental health and homecare, and after signing it, delayed dispensing the funding. These health funding agreements - which would provide desperately needed funding increases for mental health and homecare - were dismissed as “boutique” agreements not to be taken seriously. $400-million is some boutique. That was just for Manitoba - the total increase across Canada was $11-billion.
That sums up the political sleight-of-hand, however: as the Federal Liberal government transferred health funds to the provinces, conservative provincial governments refused to spend it on health, and then encouraged suffering citizens to take it out on the federal government - with considerable electoral success.
This was a communications strategy adopted by conservative premiers and further validated by the NDP in BC, since the argument was politically useful for them as well, both at the provincial and the Federal Level.
The result was a “bizzarro-world” debate where all of the salient facts had been reversed. It was a public relations coup - the premiers who were actively cutting services and cutting off access to health care successfully shifted blame to the federal government, which was actively increasing funding, sometimes for the first time in years.
It was an impressive feat of propaganda, especially given that same Conservative Premiers cutting services were responsible for significant cuts to federal health funding when they were members of parliament in a Conservative Government - including Brian Pallister and Jason Kenney.
The Ticking Time Bomb in the 2007 Budget Omnibus Bill
In their 2007 Federal budget omnibus bill, the Harper Conservatives created a ticking time bomb for Canada’s health care funding model that began in 2014.
Prior to 2014, the health care funding model took into consideration extra costs for provinces - it added extra funding based on need.
The 2007 Federal Budget, changed that formula when funding was calculated on a "strict per-capita basis.”
The result was that every province in Canada faced reduced health transfers, except Alberta, which saw a $1-billion dollar annual increase at the expense of every other procince.
The Globe and Mail article ‘The funding formula for health care is broken’, published on October 9, 2013, estimated that,
“Based on estimates for 2014-15, Alberta will receive $954-million more under the new formula than under the current formula – $235 for every man, woman and child in the province.
Every other province will lose money as follows: Ontario, $335-million; British Columbia,
$272-million; Quebec, $196-million; Newfoundland, $54-million; Manitoba, $31-million; Saskatchewan, $26-million; Nova Scotia, $23-million; New Brunswick, $18-million; and Prince Edward Island, $3-million.”
Some of the Conservative MPs who voted to cut health care in every province but Alberta were Pierre Poilievre, Maxime Bernier, Brian Pallister, and Jason Kenney.
This had an immediate impact on the budgets of provinces, who were suddenly faced with the choice of cutting back on health care, running larger deficits, or raising taxes. Sometimes, they had to do all three.
Provinces like Manitoba have higher health care costs because of a widely dispersed northern or rural populations, and the health issues that affect people living in dire poverty. Other provinces face challenges because they have older populations.
2011: Federal Conservatives Deliver Unilateral Cuts to Provincial Healthcare Funding
Another major change in federal health care funding happened when in 2011, the Harper Conservatives also moved to unilaterally change annual health care increases from 6% a year to 3%. When the provinces objected, they were told they could raise taxes.
Conservatives also put provinces on a “fixed allowance” of transfers, which meant that some provinces had total transfers capped for years. In the case of Manitoba, equalization transfers were cut.
In 2010-11, total federal transfers to Manitoba were $3.348-billion. Five years later, that total had increased to $3.359-billion. This is an increase of $11-million, which amounts to a per capita increase per Manitoban over five years of $8.50.
To repeat, over five years, the total per capita increase in funding under the Federal Conservatives was eight dollars and fifty cents.
It has to be said, this is the opposite of what the Federal Liberals did when Jean Chretien and Finance Minister Paul Martin aimed to balance the budget by reducing transfers to provinces in the 1990s, along with raising taxes.
While Conservatives and the NDP alike have railed against those fiscal measures for decades, it was implemented quite differently - namely, that the transfers to Canada’s richer “have” provinces, like Ontario and Quebec, were targeted, while poorer “have not” provinces had their equalization transfers increased to spare them.
As you can see from this graph, total federal transfers to the Manitoba Government were flat, or even declining, for six years straight, in the immediate aftermath of the Global Financial Crisis. So for six years, with a growing population, an aging population, and inflation, the province of Manitoba received no increases in transfers, as well as a cut to health care funding.
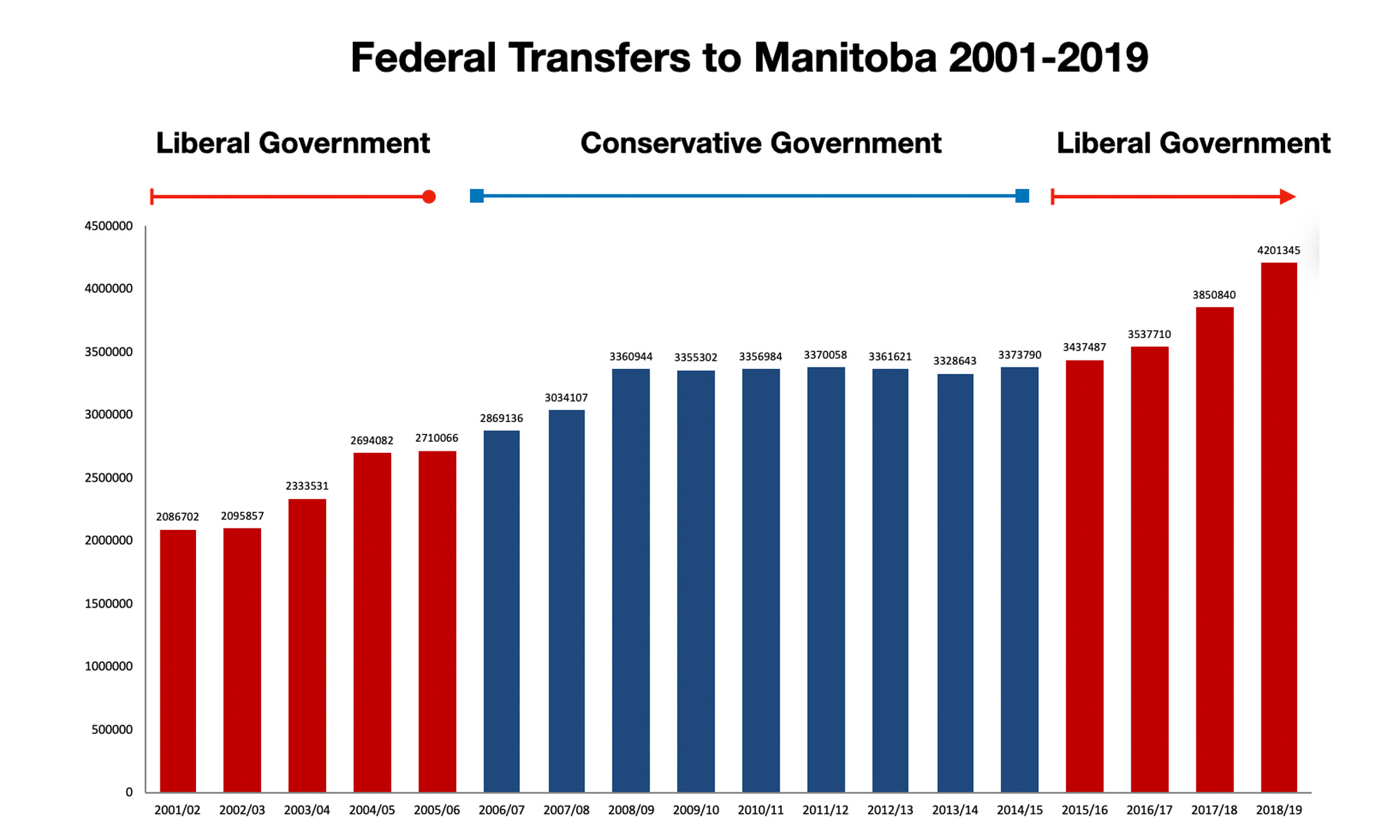
The result, unsurprisingly is that the province of Manitoba, and other provinces, were forced to borrow, cut, raise taxes, or all three. They did all three.
(While the chart says “Manitoba” it means the Manitoba Government, and does not include other Federally-funded entities in the province, like First Nations or the military.)
Since the Federal Liberals came to power in 2015, while the base rate of the Canada Health Transfer (again, CHT) has remained the same, there have been major increases in other payments that are not counted in the one stream of federal funding that is the CHT.
Provinces count on the CHT for health dollars, but that is not the only source of federal funding for health. Equalization payments can be spent on health and welfare. That is one of the reasons for equalization payments to provinces - is to “top them up” to ensure that every Canadian can get a similar level of public services for a similar level of taxation.
Equalization payments for Manitoba in 2022-23 are projected to be $2.933-billion, which is $1.195- billion more than in 2015-2016.
In the 2017 Federal Budget, the government introduced a new $11- billion health care fund. Manitoba’s share was $400-million over ten years to fund home care and mental health services. The Manitoba PC government delayed signing it for two years. This fund is a different stream from CHT.

At the same time that the federal government was ramping up investment for health care, those funds were not making it into provincial health systems. In Manitoba, from 2016-2019, the PC government capped, froze, or cut total health spending for three years straight.
While the PCs pleaded poverty for health care and blamed the federal government, they had no trouble finding the money for hundreds of millions of dollars in tax reductions, the bulk of which end up in the hands of a few.
The 50% funding claim that was only 50% true
This context is critical to the debate, and to the unanimous call by Premiers on July 12, 2022, asking to increase the current Federal contribution from 22% to 35%, based on the historic claim that the Federal Government once promised to fund health care on a 50-50 basis.
This 50% funding claim is only 50% true, and that’s important.
It might appear to Canadians, as the Premier say funding was cut from 50% to 22%, that this is something that happened recently, perhaps even by the current Federal Liberal Government, and that is the reason health care systems were such a disaster.
No Canadian should be under the impression that the Government of Canada suddenly broke a promise to fund health care in a 50-50 split with the provinces. That never happened.
Further, it’s been nearly 50 years since the agreement was renegotiated.
In 1976, the Federal and provincial governments renegotiated a new funding agreement - EPF, for Established Programs Financing “a new formula for financing the so-called "established" programs –hospital insurance, medical care and post-secondary education – was adopted.”
“At a First Ministers Meeting in 1976, Prime Minister Pierre Trudeau proposed replacing 50:50 cost-sharing with a new regime. One-half of the 1975/76 payments for 3 cost-shared programs (Hospital Insurance and Diagnostic Services Act, Medical Care Act and postsecondary education) would be paid as a block grant, escalated annually in accordance with a 3-year moving average of nominal per capita GNP growth. The other half would be offset by reducing specified federal taxes, allowing provinces to take up those revenues without any immediate changes to taxes paid by individuals and businesses.
Several provinces worried that moving from 50:50 cost sharing to block grants would expose them to unilateral federal cuts. Others agreed with federal negotiators who argued that block grants and tax points would allow provinces to reduce spending on medical services and general hospitals in favour of more cost-effective services such as home care. Ultimately, the provinces and territories agreed to a slightly more generous version of the federal proposal, embodied in the Established Programs Financing Act that took effect in April 1977.
So the new EPF funding breakdown meant that provinces would pick up 50% of the cost, and the federal government pick up 25%, with the feds permanently passing tax powers to the provinces to cover the other 25%.
People might mistakenly think that because the federal government once paid 50% and it is now measured as 22%, that federal governments had reduced the amount of money flowing into the system by 28%.
That would not be the correct conclusion - but that it what is being repeated, including by the Canadian Medical Association, which referred to the Premiers own claims, as well as by Canada’s largest union.
In 1977,
The Established Programs Financing (EPF) was introduced, replacing cost-sharing programs for health and post-secondary education. Federal funding provided through the EPF initially took the form of equal portions of a tax transfer and a cash transfer. Provinces received 13.5 percentage points of personal income tax (PIT) and 1 percentage point of corporate income tax (CIT), including some points carried over from the previous post-secondary education program. Provinces and territories received equal per capita total EPF support through a mix of cash and equalized tax points. The value of the tax points grew in line with the economy.”
This is what the change in federal funding looked like. Federal and Provincial Expenditures on Hospital and Medical Services, 1976-77 to 1988-89. The last two years of the previous funding regime were the first two lines - 1976 to 1978.

A new formula came in, and comparing it to the old one doesn’t make sense.
The reality is that the federal cash contribution to dedicated health care streams has been around 22% +/- 3-4%, since 1980. It has been rising steadily since 2016, plus increased equalization, plus health accords, plus pandemic funding, plus a new health accord.
“Triple E” Health Transfers: Equitable, Effective, Efficient
If the Federal Government restored an equitable health care funding formula tomorrow, it would not cost a dollar more, but would result in an immediate increase health care funding in British Columbia, Saskatchewan, Manitoba, Ontario, Quebec, New Brunswick, Nova Scotia, Prince Edward Island and Newfoundland and Labrador.
We need a health formula based on equity, paired with commitments from provinces that federal transfers won’t be used to subsidize tax cuts. Equity is essential to a health care formula that is efficient because funds flows to people and provinces to provide care to the people and communities that need it, not those who don’t.
A last thought: Why is health care a cost?
From time to time, a pundit will declare that it is time to have an “adult conversation” about health care in Canada, a cheap rhetorical gambit that insinuates anyone who opposes them is being childish.
We are about to be “schooled,” usually by someone who wants to claim that we are at the limits of care, that we can’t possibly afford to properly care for everyone through a public system, and that rather than expanding or improving the public system, we can expand through private care, and let “market efficiencies” deliver.
We need to make a point here, especially about the assumptions that are baked in to these conservative economic theories and philosophy, much of which are based in ideas from the 1800s, when advanced in medical
Health care is not an ordinary social service, or an ordinary service at all.
First, it makes the difference between whether people live or die, whether they can see, hear, walk, work, or see their children grow up. A per capita formula for health ignores the real and growing inequalities in our country. There are Indigenous people in Winnipeg whose life expectancy is a decade less than the rest of the community.
The change in medical and health technology over the last 150 years is mind-blowing. Miracle cures for diseases where people used to be condemned to death, being able to see into people’s bodies to see what is wrong. Restoring sight to the blind - the list goes on.
Modern medicine means people who can access health care will be treated, and/or cured, and those who cannot will die. Economics is sometimes said to be the study of allocating limited resources, but this doesn’t work with poor people with cancer.
In 1850, medicine didn’t work, and if you got sick, it didn’t make that much of a difference whether you could pay or not, because there were few effective treatments.
No anaethetic, no disinfectant, virtually no diagnostics (blood tests, imaging), no antibiotics, no effective treatments for cancer, diabetes, stroke, heart attack, and countless other ailments.
The new technologies that have been developed in the last decades include everything from hip and knee replacements, cataract replacements, organ transplants, but also all effective treatments for cancer, heart disease, diabetes, and of course preventing and protecting against infectious diseases with vaccines.
People are living longer, people who would otherwise be dead are alive, people who would otherwise be blind can see, people who could not walk. This is incredible - and incredibly positive.
So why, when we provide health care - why are these benefits ignored, when very clearly, health care is very clearly an investment that pays off.
The provision of health services in Canada is framed as being a cost and a burden to be minimized, only so long as it is public, because our conservative economic models define government as a burden that only breaks markets, when the reality is that governments make markets possible.
People can live longer, healthier able lives and there are endless examples of people’s lives or limbs and senses being saved due to what we used to call “modern medicine”.
Why don’t we recognize this?
It may be that we should divide health care into three different areas, to clarify this. Birth care, life care, and death care.
Birth care and life care seem clearly to be investments with a return.
First: birth care. It’s should be obvious that ensuring that a baby is born safely and raised in a caring environment will make a difference for that child’s entire life. It’s not a cost, it’s an investment. Pre-natal care, birth, postpartum.
Second: life care. This consists of everything else - mental health care, diagnostics, and treatment for physical ailments where people will recover - sometimes fully, sometimes partly. Some are temporary, some are chronic. Cancer, heart disease, diabetes, joint replacements and medications that help people live.
Third is “death care”. It is when people are dying that medical costs are the greatest, and death care is different. It does not, and cannot operate on a return on investment model - for it to do so would be inhumane and an affront to human dignity, and policies that are inhumane need to be challenged. Effective palliative care, however, combined with other medical treatments is a way of accepting and ensuring that people experience the end of their lives with some dignity.
The adult conversation we need to have is why Canada, as one of the richest countries in the world, can’t provide that care? Is it that we cannot provide this care, or because we choose not to?
New changes in medical technology create new moral and political issues that are incredibly disruptive. Consider the conspiracy theories around the rapid development of the Covid vaccine, which in Canada led to the Emergencies Act being declared.
In Canada’s founding Act, the British North America Act of 1867, Section 92 made the provinces responsible for hospitals, asylums, charities and eleemosynary (charitable hospitals) institutions, while leaving international quarantine, care of sick sailors, First Nations people and members of the armed services, as well as control of narcotic drugs, to the federal authorities.
Medical technology was virtually non-existent, so health care was non-existent. No one could imagine that health care technology would be so successful, and so necessary, that it would come to dominate provincial budgets 150 years later.
Who will get care? How will it be paid for? If there are many patients, but only a few treatments, how do we pick and choose who gets the care?
Medical personnel faced exactly such questions during the pandemic, as waves of sick patients exceeded the capacity of systems and personnel to care for them.
Modern economics tends to emphasize that “the market” is the best way to make these decision - but the market has never been the only way to make these tough decisions.
These are known as “lifeboat decisions” - as if you are in a lifeboat on the verge of sinking, with limited water and food, and you have to choose who will die. These are not imaginary “thought experiments” - in his amazing book, Bad Acts and Guilty Minds, Leo Katz talks about legal cases around real lifeboat situations, and how to deliver justice.
Katz says there we use four ways to allocate scarce resources - and he has great insight into why we choose them, and why some are more appealing than others.
1. The Committee — selecting people from a group of applicants
In the U.S. in the 1960s, kidney dialysis machines were in short supply, and could only handle one person at a time. LIFE magazine ran a profile on a the deliberations of a hospital committee tasked with deciding who, among a large number of candidates, would get treatment.
It came to be known as “The Seattle God Committee,” and it took a huge number of variables into account when choosing the patients who would receive treatment, going beyond their likelihood of survival to the number of children they might leave behind, their career, and more. Committee members agonized over each decision, since the choice meant that one person would live while another died.
The benefit of the committee, as Katz argues, is that it:
Preserves our sense of control and fairness because we get to make a case.
It discriminates by picking and choosing the best candidates — a poor righteous man with many children might be selected over a wealthy dilettante whose kidney damage is the result of a lifetime of binge drinking.
Its deficiency, says Katz, is that it humiliates the loser by pronouncing them inferior, because the decisions are made based on whether people are seen as deserving : “He is not just left wanting,” Katz writes, “he is found wanting.”
2. The Lottery — picking people randomly from a select group
Selecting people by lottery has the advantage that:
It doesn’t discriminate, because every person is treated equally — each person has the same chance of receiving treatment.
Its pitfall, Katz argues, is that it highlights and is open about our “social stinginess,” in that it makes it clear that we don’t have enough resources for everyone, and
Strips us of any sense of control. There is no appeal or argument to be made.
A lottery might seem like a particularly outdated or unfair way of delivering health care, but it is being used today. When U.S. states resisted the expansion of the U.S. Medicaid program under the Affordable Care Act, Tennessee, did so by adopting a lottery. A single phone number was provided and only the first 2500 callers will receive care.
3. The Market — competing for price
Katz sees that there are a number of reasons we like the market approach.
It discriminates in two ways:
Patients can pay a premium for better service or faster access, but
Service providers will also shift their practices towards patients or specializations that generate more revenue.
Because we can earn or borrow funds to get treatment, it “preserves our sense of control, doesn’t publicly humiliate, and expresses no open preferences.”
The market solution creates the illusion that anyone can get access: the only issue is money. The reality, of course is that the cost of medical treatment is such that most people will be unable to afford care without either private or public insurance.
“No wonder,” writes Katz, “[the market] is so often used or recommended for making tragic choices.”
In the 1970s Arthur Okun said “The cliché should at last be validated: the market should not be able to legislate life and death.”
Except this is no longer considered a cliché - in fact, it seems like a radical assertion, albeit of common sense.
If health care isn’t a cost, what is it?
If we want change, we need to start by changing the way we look at things.
One of those changes is the recognition that public investments in health care, education and infrastructure are just that - they are investments, not costs. Simon Patten was the first professor of economics at the Wharton Business school, and he had ideas that were startlingly different from the way we think today.
[Patten] “wanted the government to provide universal public goods: a “well-organized system of public education, public parks, cheap, yet elevating places of amusement, good public roads in the country, and an efficient system of drainage and sanitation in the cities.”
Such expenditures would raise industrial productivity and the general standard of living in the same stroke. “The test of a good tax is that it creates more wealth than it destroys,” he posited in The Theory of Dynamic Economics. “If the courts, post office, parks, gas and water works, street, river and harbor improvements, and other public works do not increase the prosperity of society they should not be conducted by the State.” Patten argued that not only were such public investments prudent, they amounted to an additional factor of production, along with capital, labor, and land. They “improve the health and intelligence of all classes of producers and thus enable them to produce more cheaply, and to compete more successfully in other markets.”
Health care, education, and public infrastructure are not costs: in addition to capital, labour and land, they are an additional factor of production that contribute to the common wealth of society.
That’s why public health care matters, and why building a stronger and more responsive health system in Canada starts with a basic principle: the funds need to go to where they are needed most. Equity matters. And so does recognizing real value, whether it is public or private.
Can every Canadian pendant please stop equating what’s going on in individual provinces in this country and extrapolate it to me and that’s what’s happening everywhere in Canada! It’s NOT THE SAME . It’s different in every bloody province.
I’m not sure why I keep having to say this, but the Canada Health Transfer is a federal program that provides financial support to provinces and territories for healthcare. Once that money is in the provinces hands, that’s it, that province is responsible for the services rendered for that money in their province.
It is not Canada’s healthcare debate. It is every provinces healthcare debate.